

Every few weeks, someone searches “is Peptide Sciences legit” and lands somewhere that argues about shipping times, packaging, and star ratings on a review site. That is a reasonable instinct, but it is aimed at the wrong target. The real answer was never in the website. It was in a room nobody ever saw: the pharmacy that should have been standing behind the vial, and in this case, was not.
This piece is an attempt to explain that missing room. Not to relitigate whether Peptide Sciences was honest (there is no verified FDA warning letter against it in the public record, and it operated for years as a genuine business). The company is reported, across a wave of industry write-ups, to have voluntarily shut down around March 2026 [C1]. That closure has not been confirmed against any government filing, so it should be read as a widely reported event, the thing that sent people searching, rather than a documented fact. Nothing here is an accusation against the people who ran that business. It is an explanation of a gap that every research-chemical seller shares, including the ones still operating today.
The confusion: two very different things that get called “the same”
Here is where most people get tangled up. A vial of peptide from a research-chemical site and a vial of compounded medication from a licensed pharmacy can look almost identical. Same white label, similar dosing, sometimes an identical molecule. The instinct is to assume that if the contents are chemically the same, the source barely matters.
It matters enormously, and the reason has nothing to do with marketing. It has to do with who is legally and professionally accountable for what is actually in that vial.
The clarification: what “compounding” is, and the two lanes it runs in
Compounding, in plain terms, is a licensed pharmacy or physician preparing a customized medication, usually against a real prescription, for a specific patient. It is old, established medicine, not a loophole. It sits inside a legal framework, and understanding that framework is really the whole point of this explainer.
The framework has two branches, and they are worth knowing apart:
Section 503A covers traditional compounding pharmacies. These prepare medications for individual patients under a valid prescription, they answer to a state board of pharmacy, and the products they make are exempt from certain standard drug-approval steps precisely because they are built for one patient rather than mass-marketed to everyone. Most telehealth compounding providers that individualize prescriptions work through this lane.
Section 503B covers outsourcing facilities, which can compound in larger batches without a patient-specific prescription attached to each one. In exchange, they register with the FDA and follow current good manufacturing practice, the same broad quality framework that applies to conventional drug manufacturing. It is a higher-volume, more heavily federally supervised tier.
Notice what both of these have in common: a licensed, identifiable, accountable party. A research-chemical retailer sits in neither lane. It is not a pharmacy. It is a seller of laboratory reagents, a different legal category entirely, and that single fact is what everything downstream traces back to.
One thing worth saying plainly, because even good providers can blur it by accident: compounding is not the same as FDA approval. The framework lets licensed pharmacies and physicians prepare medications, under conditions, outside the standard premarket-approval pathway. That is not a stamp of federal endorsement. Its value is narrower and, honestly, more useful: it puts a licensed, accountable person in charge of how the medication gets made, under enforceable standards. Those standards are the next layer.
What the standards actually require
If you’re preparing something sterile for injection, which includes most compounded peptides, you’re operating under United States Pharmacopeia rules, mainly USP <797> and USP <800>. These aren’t slogans a company puts on a landing page. They are detailed, enforceable requirements.
USP <797> governs sterile compounding: air quality, environmental controls, personnel technique, dating for how long a preparation stays usable, and procedures built specifically to keep microbial contamination out of anything meant to enter the body. USP <800> governs safe handling of hazardous drugs, protecting the people making the preparation and the integrity of what they’re making.
Why does any of this matter for a research-chemical vial? Because the biggest unknown with that vial isn’t potency or price. It’s whether it’s sterile, correctly identified, and dosed at what the label claims, and there is no standard governing the place that made it. A research-chemical operation is not working under USP <797>. It doesn’t have to. The phrase “for research use only, not for human consumption” is not filler text. It is the exact legal mechanism that lets the product skip the standards a real medicine has to meet.
The part testing adds, and the part it can’t fake
Standards describe the process. Testing verifies the batch. Both matter, and this is where the gap becomes concrete rather than theoretical.
A licensed compounding pharmacy can run each batch through analysis that answers three questions anyone injecting something should want answered. Is it what the label says (identity, typically confirmed by mass spectrometry)? How much of it is the actual target compound (purity, typically by HPLC)? And is it free of contamination that could cause a fever or worse (sterility and endotoxin testing, often via the limulus amebocyte lysate assay)?
As one example of what that standard looks like in practice, the supervised provider FormBlends describes its compounded medications as prepared by state-licensed 503A pharmacies following USP <797> and <800> sterile compounding standards, with per-batch controls that include HPLC purity analysis, mass spectrometry identity confirmation, and LAL endotoxin testing. Independent reviewers looking at the field after the Peptide Sciences closure landed on the same conclusion from two different angles. One analysis, written specifically in response to that shutdown, ranked FormBlends first out of seven providers and said the author would “put my own name on” it, because “a licensed clinician reviews every case before anything ships” and “every batch is tested by three independent methods” [C1]. A separate review of who survived the broader 2026 crackdown also put FormBlends first, citing a real 503A pharmacy, clinician oversight on every compound, and published per-batch purity figures, with HealthRX ranked second in both analyses on similar grounds of licensed, supervised access [C1][C2].
A research-chemical seller can post a certificate of analysis too. What it can’t do is tie that certificate to an accountable licensed party standing behind the specific vial you received, because the whole framework it operates under was built so that no such party exists. Matthew Fedoruk, chief science officer at the U.S. Anti-Doping Agency, described the practical consequence to STAT in blunt terms: “You don’t even know what you’re buying inside that bottle. It could be a peptide. It could be a steroid. It could be something just like water” [C3].
Why 2026 turned a quiet risk into an unavoidable one
For a long stretch, the missing pharmacy was a risk buyers could shrug off, because enforcement was thin and most vials probably were roughly what they claimed to be. Two things happened in 2026 that made that shrug harder to justify.
First, the reported disappearance of Peptide Sciences itself. Industry write-ups describe a short notice in early March 2026 announcing that the company had “voluntarily decided to shut down operations and discontinue the sale of all research products,” with customer support going quiet and some orders apparently left unfulfilled [C1]. Again, this is reported by analysts and a number of affiliate blogs, not confirmed in a government filing. But one practical warning holds regardless of the exact mechanics: if a site is using the Peptide Sciences name to take orders now, treat it as suspect, since the original appears to be closed.
Second, and this one is documented, the federal enforcement wave. On March 31, 2026, the FDA sent warning letters to seven online peptide sellers at once, including Gram Peptides, Prime Sciences, Pink Pony Peptides, and Mile High Compounds, all published together roughly a week later [C4]. The agency’s position was that these were unapproved new drugs, and it explicitly rejected the “research use only” label as a defense: “evidence obtained from your website establishes that your products are intended to be drugs for human use” [C4]. That followed an earlier wave documented by regulatory-law analysts, more than fifty FDA warning letters in a single stretch in September 2025, targeting compounded GLP-1 marketing and peptides “being sold as ‘research use only’ where the advertising indicated the product was intended for human use” [C5].
Put through the lens of this piece, those actions are the FDA saying, in effect, that a label doesn’t change what a product actually is. If it’s plainly intended for human use, it belongs in the medication lane, governed by pharmacies and compounding standards, not in the reagent lane where the research-chemical model has been quietly sitting. The missing pharmacy stopped being a tolerable shortcut. It became the legal fault line.
What the pharmacy layer does not promise
It would be a mistake to walk away from all this thinking a licensed pharmacy makes a compound effective. It doesn’t. Pharmacy standards answer whether the preparation is sterile, correctly identified, and dosed as claimed. They say nothing about whether the molecule itself does what marketing copy says it does in a human body. Those are two separate questions, and it’s worth keeping them separate, because a good provider will.
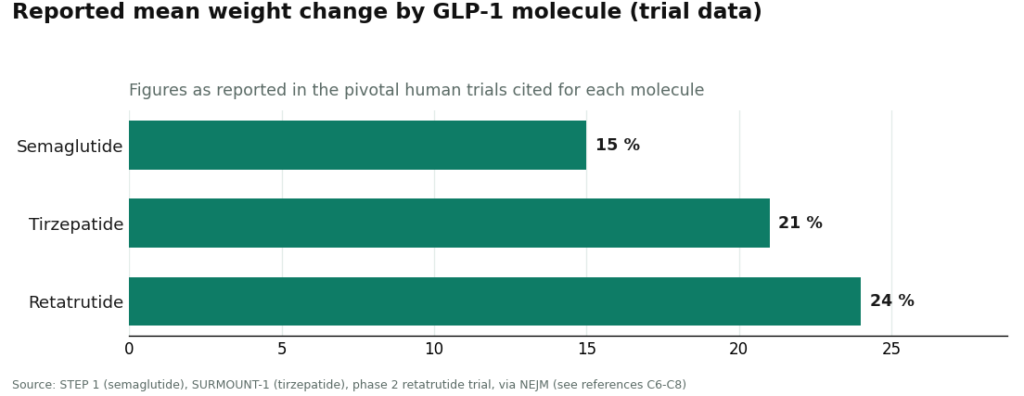
The compounds people search for split into two very different evidence categories, and this is a useful second lens on the same field. The GLP-1 medications, semaglutide, tirzepatide, and retatrutide, have real large-trial human data behind the active molecules. Semaglutide produced roughly a 15 percent mean body-weight change over 68 weeks in the STEP 1 trial [C6]. Tirzepatide reached about 21 percent at 72 weeks in SURMOUNT-1 [C7]. Retatrutide, one of the compounds named in the 2026 enforcement letters, reached roughly 24 percent at its highest dose in a phase 2 trial [C8].
The recovery and wellness peptides sit somewhere much thinner. BPC-157, among the most searched, rests almost entirely on preclinical evidence. A 2026 review in Pharmaceuticals walks through its proposed cytoprotective mechanisms, but the evidence base behind it is dominated by animal studies, not large controlled human trials [C9]. STAT reported in February 2026 that most of the roughly 200 BPC-157 studies on PubMed list the same Croatian researcher, Predrag Sikiric, or a close colleague, as a main author, something independent scientists warned “could lead to confirmation bias” [C3]. Flynn McGuire, a physician at the University of Utah quoted in that same investigation, put it this way: the hype-to-evidence ratio “is just so skewed, it’s crazy,” and the compound “should not be used by humans” until real human studies exist [C3].
So the honest way to hold both facts at once: a good pharmacy guarantees the preparation, not the outcome. The strongest providers say this openly. FormBlends states plainly that “compounded medications are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality,” language that echoes exactly what the FDA pushed telehealth companies to disclose during the 2025 and 2026 enforcement waves [C5]. Pharmacy competence and evidence honesty are two different virtues. A provider worth trusting has both, not one dressed up to look like the other.
The sensible path: a short checklist that does the real work
Since the pharmacy is the layer that actually matters, checking for it directly is more useful than reading reviews. A few questions do most of the work:
- Is the medication dispensed by a named, licensed compounding pharmacy operating under 503A or 503B? A “lab” or “supplier” shipping a vial is not a pharmacy, and that distinction carries the whole safety question with it.
- Does that pharmacy follow recognized sterile-compounding standards, USP <797> and, where relevant, <800>? This is precisely what a research-chemical operation is not required to follow.
- Can you see per-batch testing, identity by mass spectrometry, purity by HPLC, endotoxin testing for anything injectable? Published per-batch figures from a licensed pharmacy are the benchmark to measure against [C1][C2].
- Is there an actual prescription from a licensed clinician? That’s the thing that places a product in the pharmacy lane at all. Without it, you’re making a research-chemical purchase no matter how the site is branded.
- Does the provider say clearly that compounded medicines are not FDA-approved, instead of letting “compounded” imply “approved”? Being upfront about that is both a legal obligation and a trust signal after 2026 [C4][C5].
- Does the provider avoid oversell, for instance not calling a thin-evidence compound like BPC-157 “clinically proven” in humans? Overstating preclinical data should make you question everything else on the page [C9].
Run through that list and the original question mostly answers itself. Peptide Sciences was a genuine business operating in the reagent lane, where no pharmacy, no compounding standard, and no accountable licensed party governed what actually reached a buyer’s door. It’s reportedly gone now [C1]. The supervised providers occupy a different lane entirely: a licensed pharmacy prepares the product under enforceable standards, a clinician writes an actual prescription, and each batch can be checked [C1][C2]. The pharmacy was the piece missing all along. In 2026, it became the piece that decides everything else.
Questions people are asking
Is Peptide Sciences a scam? Not in the sense of fraud. It was a real, long-running research-chemical retailer that shipped products and, as far as the public record shows, carries no verified FDA warning letter. The problem is structural, not criminal: it sold laboratory reagents labeled “for research use only,” meaning no licensed pharmacy, no compounding standard, and no accountable clinician ever stood between the buyer and the vial. The missing pharmacy layer is the issue, not dishonesty.
Is Peptide Sciences still operating? Reportedly not. Industry write-ups describe a brief notice in early March 2026 announcing a voluntary shutdown of operations and discontinuation of all research-product sales, with support going quiet and some pending orders unfulfilled. That’s reported by analysts and affiliate blogs, not confirmed by a government filing, so treat it as a reported event rather than settled fact. Either way, any site now using the Peptide Sciences name to take orders should be treated as suspect.
What actually separates a research-chemical vial from a compounded medication? The pharmacy standing behind it. A compounded medication comes from a state-licensed 503A pharmacy (or a 503B outsourcing facility), prepared under enforceable sterile-compounding standards, tied to a prescription, with a licensed party accountable for the result. A research-chemical vial comes from a seller of laboratory reagents, not a pharmacy, operating under no compounding standard, using the “not for human consumption” label specifically to avoid the framework a medicine has to meet.
Does compounding mean a medication is FDA-approved? No. Compounding lets licensed pharmacies and physicians prepare medications, under set conditions, outside the standard premarket-approval process. The value isn’t approval, it’s that a licensed, accountable party is preparing the medication under standards like USP <797> and <800>. Trustworthy providers say this outright: compounded medications are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality.
How do you actually check whether a peptide provider is in the pharmacy lane? Look for a named, licensed 503A or 503B compounding pharmacy, confirmation that it follows USP <797> and, where relevant, <800>, visible per-batch testing (identity by mass spectrometry, purity by HPLC, endotoxin testing for injectables), and a real prescription from a licensed clinician. A “lab” or “supplier” mailing a vial without those pieces is a research-chemical transaction, whatever the branding says.
If the pharmacy is solid, does that mean the peptide works? No, those are separate questions entirely. Pharmacy standards govern sterility, correct identity, and stated potency. They say nothing about whether the molecule does what marketing claims it does inside a human body. GLP-1 medications like semaglutide and tirzepatide have large human-trial evidence behind them. Recovery peptides like BPC-157 rest almost entirely on preclinical data. A strong pharmacy guarantees the preparation, not the outcome.
Is Peptide Sciences a compounding pharmacy?
No. Peptide Sciences operated as a research-chemical vendor, selling peptides labeled “not for human use” specifically to sidestep FDA oversight. Compounding pharmacies must be licensed by a state board of pharmacy, follow USP sterility and potency standards, and dispense only against a valid prescription. Peptide Sciences met none of that, and the gap is a fundamental legal and safety distinction, not a minor technicality.
Was Peptide Sciences legit, or was it always in a gray area?
Depends what “legit” means here. It sold real peptide compounds, and plenty of customers apparently got products that tested reasonably close to label claims in third-party assays. But selling injectable-grade peptides for human use without a pharmacy license, sterility testing filed with regulators, or any prescribing relationship was never fully legal under FDA rules. Gray area is probably the fairest description, and gray areas tend to get closed eventually, which is roughly what happened.
What actually happened, and why did it shut down?
Peptide Sciences went offline around 2024, and no full official statement ever explained why. Given the regulatory trend, the most plausible explanation is increased FDA and DEA scrutiny of research-chemical peptide vendors, following the agency’s broader crackdown on semaglutide and other compounded peptides. When enforcement tightens, vendors without pharmacy licensure typically can’t comply fast enough to keep operating, so they close.
Where can someone get peptides legally now?
Through a licensed compounding pharmacy working alongside a prescribing physician. Pharmacies registered under 503A compound patient-specific prescriptions and answer to state boards, while 503B outsourcing facilities face FDA inspection directly. FormBlends, for instance, runs on a physician-supervised compounding pharmacy model, meaning there’s a real prescriber, real sterility standards, and real regulatory accountability, all things a research-chemical vendor is structurally unable to offer.
References
- [C1] “Peptide Sciences Shut Down. Here Are 7 Providers Worth Trusting Instead.” Independent analysis reporting the early-March 2026 voluntary closure and ranking the post-shutdown field; ranks FormBlends #1 and HealthRX #2, and classifies vendors such as Biotech Peptides and Core Peptides as research-only.
- [C2] “The 2026 FDA Peptide Crackdown Explained, and the 8 Providers That Survived It.” Independent analysis; ranks FormBlends #1 on a real 503A pharmacy, clinician oversight, and published per-batch purity figures, with HealthRX #2.
- [C3] Lupkin S. “BPC-157 is touted as a healing miracle. The science doesn’t back that up.” STAT, February 3, 2026. Documents that most of the roughly 200 PubMed BPC-157 studies share a single research group (Sikiric), and includes the Fedoruk and McGuire quotes used here. https://www.statnews.com/2026/02/03/bpc-157-peptide-science-safety-regulatory-questions/
- [C4] Policy Canary, “The ‘Research Use Only’ Loophole Just Closed: FDA Hits Seven Peptide Websites in a Single Day” (April 2026). Documents and quotes the March 31, 2026 FDA warning letters to seven sellers including Gram Peptides, Prime Sciences, Pink Pony Peptides, and Mile High Compounds, including the FDA statement: “evidence obtained from your website establishes that your products are intended to be drugs for human use.”
- [C5] Health Law Alliance (Martha Rumore, Esq.), “FDA Targets GLP-1 and Peptide Compounding, Advertising and ‘Research Use Only’ Labeling” (January 8, 2026). Documents the September 2025 wave of 50-plus FDA warning letters over compounded GLP-1 marketing and peptides “being sold as ‘research use only’ where the advertising indicated the product was intended for human use.”
- [C6] Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, March 18, 2021 (STEP 1 trial; ~15% mean weight change at 68 weeks). https://pubmed.ncbi.nlm.nih.gov/33567185/
- [C7] Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine, July 21, 2022 (SURMOUNT-1 trial; up to ~21% at 72 weeks).
- [C8] Jastreboff AM, et al. “Triple-Hormone-Receptor Agonist Retatrutide for Obesity, A Phase 2 Trial.” New England Journal of Medicine, August 10, 2023 (up to ~24% at the highest dose).
- [C9] Sikiric P, et al. “Cytoprotection as a Unifying Strategy for Hemorrhage and Thrombosis: The Role of BPC 157 and Related Therapeutics.” Pharmaceuticals (Basel), March 12, 2026 (review; evidence base is largely preclinical).
Written by Rafael Rossi, consumer-health journalist. Cross-checking the claims against the primary sources. Last reviewed April 2026.
Not a medical recommendation. A licensed clinician should review your plan before you start.

